A Professional Networking Site for Doctors & Medical Students Worldwide

Quadriplegia - ( clinical aspects of)-For the benefit of medical students
Quadriplegia
Paralysis affecting all 4 limbs.
Synonym: Tetraplegia
Partial loss of power is Quadriperesis/tetraperesis
Types: I. Quadriplegia of upper motor Neuron Lesion
II. Quadriplegia of lower motor neuron lesion.
II. Lower motor lesion: Flaccid quadriplegia
CLASSIFICATION (According to the site of lesion)
SITES:
Anterior horn cells/Roots/peripheral nerves/Myoneuronal junction/Muscles.
✿Lesions of anterior horn cells:
Acute anterior Poliomyelitis
✿Lesions of Roots:
Guillain-Barre Syndrome
✿Lesions of Peripheral Nerves
Polyneuropathy
- Porphyria
- Diphtheria
- Infective hepatitis
- Infectious mononucleosis
- botulism
✿Lesions of myoneuronal junction:
Myasthenia gravis
✿Lesions of Muscles:
Myopathy
a) Genetic
b) Non genetic
Periodic paralysis
Spastic Quadriplegia
Sites of Lesion:
High cervical cord/Brain stem/Cortex
- HIGH CERVICAL CORD LESION
- Trauma
- i. Fracture dislocation of cervical spine
- ii. Hematomyelia
- Cervical spondylosis
- Cervical cord tumor
- Cranio vertebral anomalies
- i. Klippel-Feil syndrome
- ii. Arnold chiari malformation
- iii. Platy-basia
- BRAIN STEM LESION
- VBI-vertibro basilar artery insufficiency
- Bulbar poliomyelitis
- Syringobulbia.
- Disseminated sclerosis
- Motor neuron Disease
- CORTICAL LESIONS
- Cerebral palsy
- Diffuse sclerosis
- Hydrocephalus
- Birth injuries
- Defects in brain during fetal development
QuadriplegiaPredominantly involving proximal group of muscles
Conditions causing:
1. Poliomyelitis –Anterior horn cells
2. Spinal muscular atrophy
genetically determined disease of motor neurons
3. Guillain –Barre Syndrome(GBS)
4. Periodic paralysis, Myotonia
5. Myopathy
6. Myasthenia
7. Diabetic Mononeuritis multiplex
(Sciatic and femoral nerve)
8. Diabetic myopathy
-involving proximal shoulder, pelvic girdle muscles
-unilaterally or bilaterally.
Predominantly involving distal group of muscles
1. Distal Myopathies
2. Peroneal muscular atrophy.
3. Polyneuropathies.
-Multiple symmetrical peripheral neuropathies
(Alcoholism, diabetes, carcinoma, lead poisoning)
4. Mononeuritis multiplex
-Asymmetrical involvement of peripheral nerves.
(-Leprosy, Amyloid, PNA, neurofibroma)
Differential Diagnosis of Quadriplegia.
I. AS PER NEURO ANATOMICAL SITE OF LESION
- Anterior Horn cells
- Weakness, wasting, fasciculation.
- Fasciculations occasionally in root lesios
- Peripheral nerves
- Distal distribution, sensory involvement, absent reflexes.
- Neuromuscular junction
- Predominant ocular and bulbar muscle involvement.
- Diurnal variation.
- Reflexes preserved.
II. TENDON REFLEXES AND QUADRIPLEGIA
- Preserved in myopathy
- Absent in Spinal muscular atrophy, Polio.
- Areflexia in GBS.
III.Diagnosis according to chronological evolution
- Acute onset
- Guillain –Barre
- Periodic paralysis.
- Subacute onset;
- Inflammatory polyneuropathies.
- Guillain- Barre.
- Inflammatory polyneuropathies.
2. Diphtheria
3. Porphyria
4. Toxic neuropathy.
5. Rarely- myasthenia
6. Toxic myopathy.
7. Endocrine myopathy.
IV. Diagnosis according to progression of the disability
- SLOWLY PROGRESSIVE.
i) Over weeks to months
Polymyositis, Dermato myositis.
ii) Over years
Spinal muscular atrophy
(Werdnig- HoffmanSyndrome, Kugleberg welander
Syndrome)
Myasthenia
Muscular dystrophies.
- SLOWLY PROGRESSIVE BULBAR WEAKNESS
Anterior horn cell Disease.
- Neuro muscular junction.
Less common- Myopathy
Oculopharyngeal
Polymyositis.
Dermato myositis.
- D. SLOWLY PROGRESSIVE DISTAL WEAKNESS.
- a. Peripheral nerve lesion.
- b. Distal myopathy.
Congenital myopathy - rare
- c. Myotonic dystrophy.
- d. Fascio scapulohumeral can present with
-Distal weakness along with proximal.
V. Differentiation by certain presentations
- a. Ocular weakness and ptosis
Never in M.N.D./peripheral neuropathy / Eaton Lambert’s-no ocular or bulbar involvement.
- b. Ocular muscle weakness typical in –
Myasthenia, Myotonia.
Others:- Oculo pharyngeal dystrophy
Diabetes with Mononeuritis multiplex.
- c. Only ocular weakness.
Progressive external ophthalmoplegia
Kearns –Sayer Syndrome.
d. Episodic Weakness
Periodic paralysis
Myasthenia Gravis
Eaton-Lambert’s Syndrome-No weakness of ocular /bulbar muscles.
Recurrent temporary flaccid paralysis.
- Myasthenia gravis
- Potassium deficiency.
- periodic paralysis.( familial, Hypokalemic, Hyperkalemic)
- Primary aldosteronism.
- Disseminated Sclerosis.
- Sarcoidosis.
7. Hypothyroidism/ Hyperthyroidism
8. Porphyria
Spastic Quadriplegia (pyramidal tract involvement in)
/Spinal cord lesion/ Brain stem lesions/cerebrallesions
Spastic diplegia-All 4 limbs are affected but lower limbs are affected more than upper limbs.
- Cerebral palsy/central pontine myelinosis
CAUSES OF QUADRIPLEGIA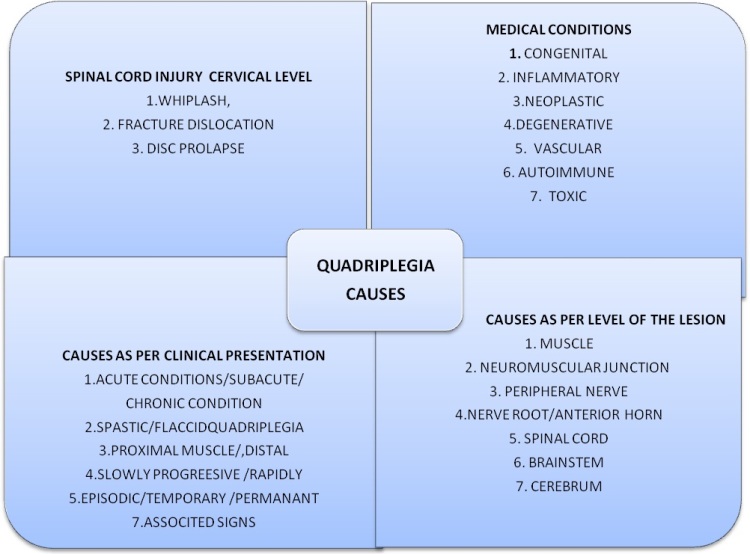
ASSESSMENT
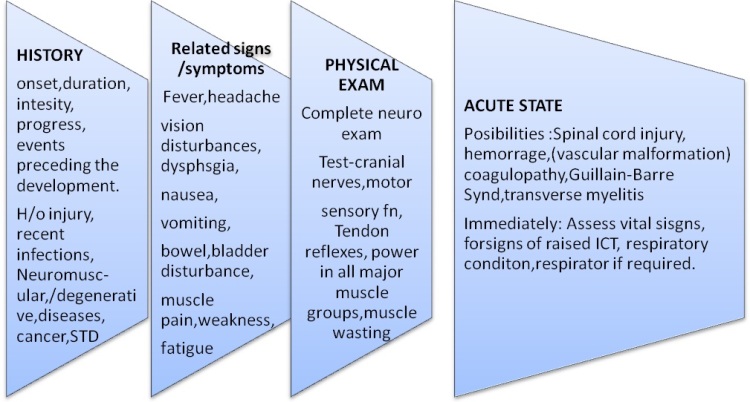
Depends on site of suspected pathology
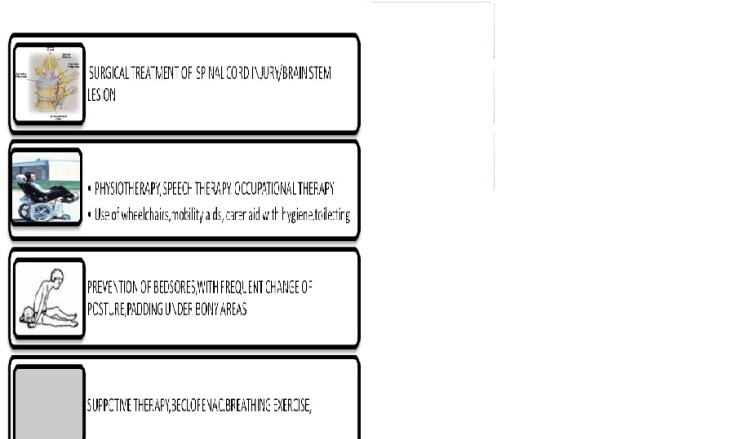
TREATMENT:
------------------------------------------------------------------------
----------------------------------------------------------------------------------------------------------------------------------------
Views: 47
Comment
Photos





Medical Videos

-

SFHFT Annual Conference
Added by Jo Joseph




-

VirtualEcho in action
Added by MedicalWorksEG
-

Back Pain
Added by Dr.A.Mohan Krishna
NEJM Jobs
© 2017 Doctors Hangout | About DH
Powered by![]()

You need to be a member of DoctorsHangout.com to add comments!
Join DoctorsHangout.com